Educational program on electrical injuries (part two): Longrid about first aid and resuscitation
By popular demand, we are talking about first aid in case of electric shock. Let me remind you that we deliberately touched on this topic in connection with the frequent reports in the media about electrical injuries received when using smartphones, headphones and other gadgets. The manuals, articles and textbooks offer various algorithms and methods for providing such assistance. This creates problems for people who provide help, who sometimes can’t decide how to actually do it right. The situation once again demonstrates that medicine is the second most accurate science after theology.
At the same time, most people want to clearly understand “how to” and “how effectively”, and not think out and argue about the author of which manual is right and whose teacher. Under the cut, a longrid is waiting for you about first aid for electrical injury with a focus on cardiopulmonary resuscitation (which is most confusing). It will be hard to push everything into one article, so at the moment we will manage first aid for adults, I will dedicate one more material to age features.
For those who are too lazy to read a lot, a section has been created that combines everything written in the most abbreviated form.
The sequence of actions is the most important thing that you need to know when assisting a person with an electric shock. Electric shock often results in death, and failure to follow the sequence of actions leads to several deaths or serious consequences for several people at once. For example, as happened in Mexico last year in the video below:
The video contains shots that kill people, which may affect the mental state of children and sensitive adults.
The main thing that the described sequence is aimed at is to minimize the probability of hitting the one who is helping. Let's start by the points:
Discharge from the current
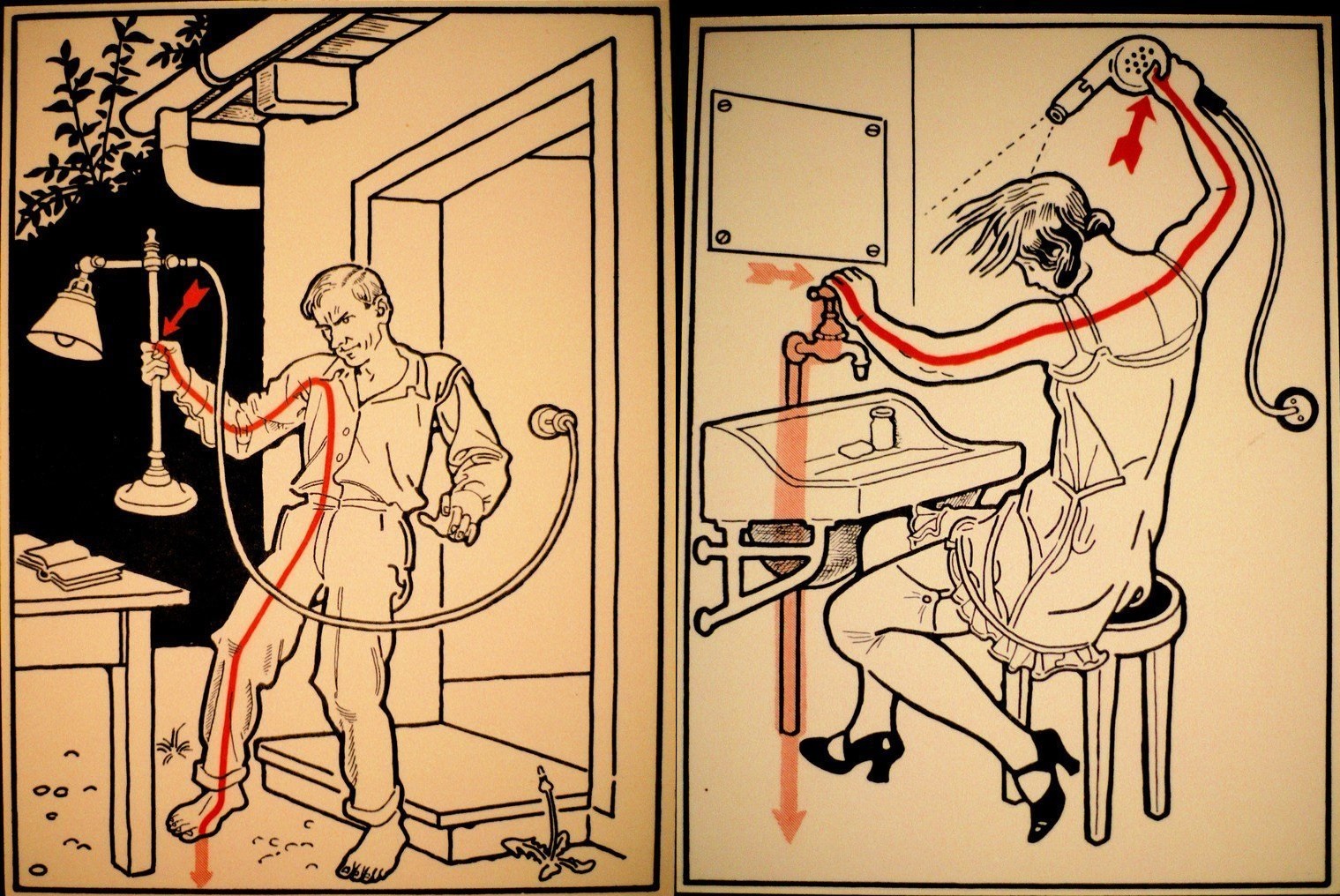
Stop the effect of the electric current on the victim by disconnecting the
current source. If it is impossible, remove the conductor from the victim using dry (!) Objects created from dielectrics. It is important to remember that the classic example with a stick or mop, which is in some benefits, is not very good, due to the fact that mops are wet, as well as wood lying on the ground.
Ideally, the use of dielectric gloves, which are considered the ideal way to protect against voltage up to 1 kV, which is consistent with the electrical shock from household appliances and charging gadgets. When talking about a higher voltage, and as a consequence of a more serious current (high-voltage lines, industrial electrical installations, substations), it is necessary to use dielectric bots and a dielectric mat.
In some recommendations it is advised to wear dry wool or household rubber gloves, rubber boots, you can additionally put insulating material (rubber mat, board) under your feet, then remove the conductor from the body with a dry dielectric or clothes
It is also recommended that the victim be struck at least 4-5 meters in case of a household electrical shock (voltage up to 1kV).
If the mains voltage is more than 1 kW (break of a power line wire, for example), if you do not have the appropriate tolerance (and at the same time a set of dielectrics), you should not approach the victim closer than 8 meters. It is necessary to call the Ministry of Emergency Situations and the ambulance, and, if possible, warn others about the danger. On the topic of what is better to remove the conductor from the body of the victim, when there are no special tools, you can write a dissertation. For those who have a great desire to delve into the topic, I recommend first to get acquainted with what electric
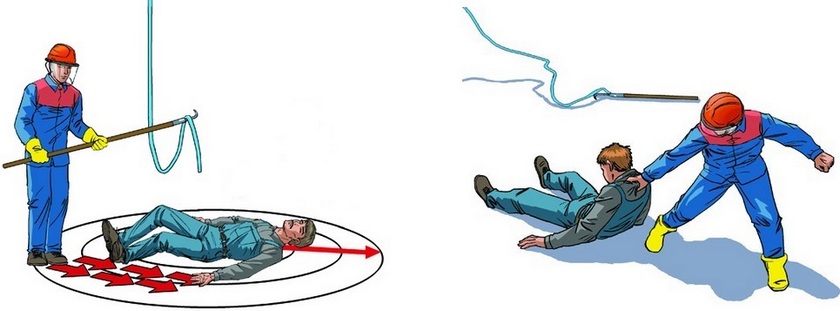
Also, in extreme cases, the source can be cut off (for example, wires) with an ax with a dry dielectric handle.
dielectric strength . Understanding the electrical strength of the materials from which the objects around you are made, and knowing the characteristics of the current, you can easily find a suitable object.
It is also important to understand that turning off the source causes the light to go off. This should be taken into account when assistance is provided in the dark or in a room without natural light.
Examination (pulse, respiration, consciousness, bleeding, burns)
After the release of the current, you should call the ambulance and conduct an inspection of the victim. The main thing in this examination is to assess the state of functions, without which the victim can not live - this is blood circulation (pulse first on the carotid, and if available - on the radial artery) and respiration (can be determined by chest excursions, fogging of glasses or mirrors, listening, tactile sensation air movement).

determination of the pulse on the carotid artery
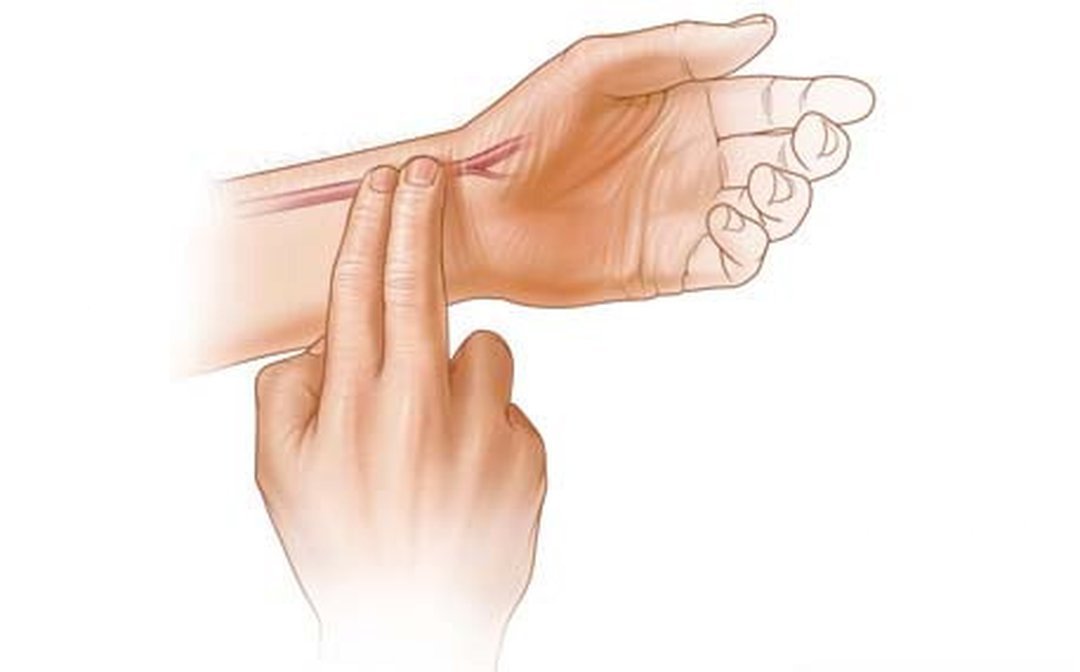
determination of the pulse on the radial artery
Also, during the initial examination, the presence of consciousness is assessed, which is not so important for life, but can provide substantial information about the severity of the victim's condition. You can try to bring the affected to the feelings with the help of ammonia. If, even from a foul-smelling liquid ammoniac, a shock struck did not regain consciousness, then we most likely deal with a severe defeat. In this state, clinical death (cardiac and respiratory arrest) can occur at any time and the victim needs increased attention to his vital functions (pulse, breathing).
Moreover, a number of authors write that after an electric shock there are long-term effects and, against the background of external well-being, cardiac arrest may suddenly develop (which is probably due to the defeat of His bundles). Therefore, it is extremely important to constantly monitor the condition of the affected before the ambulance arrives. Even if he is conscious and looks like a slightly excited "hearty".
If there is no pulse and (or) breathing - talking about clinical death, you must immediately proceed to cardiopulmonary resuscitation (which I will write in detail in the next section). It is important to begin resuscitation in the first minutes after the onset of clinical death (cessation of blood circulation and (or) respiration). After 5 minutes, irreversible changes occur in the cerebral cortex.
Also interesting is the case when the pulse is only on the carotid artery (on the neck), but not palpable on the radial (on the wrist). This is an extremely deceptive state, which indicates decompensated shock and a drop in blood pressure below 60 mm. Hg Art. In such a situation, it is necessary to prepare for cessation of breathing and (or) cardiac activity, after the onset of which it is logical to begin cardiopulmonary resuscitation.
Bleeding
If breathing and pulse is present, it makes sense to pay attention to the presence of bleeding, which sometimes happens with electric shock. Electric shock rarely leads to heavy bleeding, most likely it will be capillary or venous bleeding at the points of entry and exit of the discharge. Venous requires stopping with a pressure bandage. The capillary stop itself, but in order not to infect the wound, you should (if possible) close it with something sterile, for example, a bactericidal adhesive plaster.
Burns
Burns may also be present on the skin. If the burn surface occupies a large area and causes intense pain, it must be cooled with a large amount of water (it is important to do this at a safe distance from the current source). In the future, burns should be possible to close with something sterile, a bandage, for example. It is important not to tear off the pieces of burnt clothing, if any, but to leave them in place by closing the bandage along with the affected tissue.

Fractures and dislocations
As we found out in the previous article, mechanical injuries are quite likely in the event of electric shock, and may appear from both indirect and direct action of the current. That is, if the affected person did not fall from a height and did not beat all parts of the body against the floor, this does not mean that he cannot have a fracture or dislocation.

On examination of a fracture, there may be evidence of tissue swelling, limb deformity, a hematoma at the fracture site, and pain itself. About sprains usually says pain, pathological (not normal) mobility in the joint, deformity in the joint area. Fractures and dislocations must be immobilized - that is, immobilize, most likely an ambulance will do this. If you intend to encounter a mechanical injury if an electric shock occurs outside the exit area of an ambulance brigade, read more about transport immobilization.
General events
Also, the affected person must be drunk hot (not to be confused with feverish), give a blanket (avoid heat loss as in a state of shock), and offer validol as a placebo. It is also important to provide psychological rest, if the injured core with arrhythmia and complains of an attack, you should help him find antiarrhythmic, prescribed by a doctor, which may be with him or nearby.
Flour choice. And which algorithm is correct?
With this theme, too, things are not as simple as they seem. Perhaps everyone has seen how the films perform indirect heart massage, while the passionate rescuers of Malibu conduct intensive and seductive artificial ventilation of the lungs by mouth-to-nose method (cross out) in the mouth. Some, probably, also managed to notice that in all films this is done differently and in most cases wrong.
All drivers were taught in driving schools the skills of elementary resuscitation, as a rule, according to the method of Peter Safar (Peter Safar), better known as ABCD. At the same time, the overwhelming majority of drivers managed to forget about what the letter combination means. Other people have been trained in different places and at different times and may know other techniques. For example, doctors who studied in the harsh 90s recall the Russian “UNIVERSAL” algorithm, someone remembers unnamed Soviet norms based on the same Safara, etc. However, when it comes to business, there is a stupor and a misunderstanding of how best to do it.
In 2010, when CPR by Safar turned 50 years old and in the same year, it was finally recognized as ineffective by modern standards, replacing it with a more advanced algorithm. In this regard, I strongly recommend that you forget everything that you remembered before and pay attention to what is accepted today by WHO and AKA (American Heart Association). In this article we will look at the CAB algorithm. I will write below about the features of the latest version of this algorithm (in a form adapted for people without special medical knowledge).
Who has a great desire to learn about the evolution of ideas about CPR, can read this article.
CAB is our all
Order of letters in the abbreviation CAB indicates the sequence in which resuscitation actions are performed:

The preparatory stage
Affected (which is already removed at a sufficient distance from the current source) should be laid on a hard, flat, dry surface. It makes sense to put something under his legs, to free him from clothes that prevent assistance. It is allowed to take off / unfasten / tear / cut clothes that make it difficult to access the chest. In this case, history knows cases when even paramedics presented financial claims for expensive linen. In this regard, some authors clarify that if you can quickly unbutton it is better to unbutton it and not cut it. After the preparatory phase, you can begin resuscitation.
Precordial punch: optional, dangerous, optional
Such a blow is the only method of mechanical defibrillation and can be effective due to the genesis of clinical death (which is often caused by fibrillation in electric shock). The automatic defibrillator is much more efficient, but, unfortunately, is not available everywhere.
Due to the trauma and high risk, the precordial blow is not used by the volunteers of the National Red Cross societies , and it was also removed from international recommendations and benefits.
At the same time, the method proved its effectiveness in the first seconds during fibrillation. To be objective, I will describe the method of application, with the proviso - the technique is really traumatic, is not included in modern algorithms for CPR, and it is the person who provides assistance for the consequences of its application.
The blow should be applied in case of a 100% certainty that there is no blood circulation, no pulse, and cardiac arrest occurred before your eyes. If you are not sure of the correctness of the strike - do not apply it and proceed to an indirect heart massage. The blow is applied with the edge of the palm clenched in the fist across the sternum, the blow must fall into place 2 centimeters above the xiphoid process of the sternum (that is, where shown in the figure). The xiphoid process itself must be palpated (grope) and be sure to close with your fingers. Only then can one strike (!) A sharp blow above the fingers (covering the process) from a distance of no more than 20 cm.

No need to bash on the sternum with all the dope in a fit of insane heroism. You can not beat from the shoulder , the main thing is not strength, but how sharply the blow is dealt. It is important to understand that during the resuscitation, the carer has a lot of adrenaline and remarkable strength appears even in fragile-looking girls.
Indirect massage - correctly 30, not 10-15
Indirect massage is the most statistically effective method of elementary cardiopulmonary resuscitation and is a compression in the same place in which the precardiac stroke was performed - strictly in the middle of the chest, 2-3 centimeters above the xiphoid process . It is important not to move your hands to the right or left, in such cases it is easy to damage the ribs, and the rib cage fragments of the ribs are easily damaged.

Location of an indirect massage
Compression when performing an indirect massage is performed with the base of the palm of one hand, the other presses from above, the fingers are raised to eliminate pressure on the ribs. The important point is that the arms should be straightened, flexion in the elbows is not allowed. The depth of the compression movements should be 5 cm. At this depth, it is possible to squeeze the heart to provide sufficient blood pressure to supply blood to the brain.

There is a lot of discussion about the frequency with which compression should be performed. Modern algorithms assume a series of 30 compressions alternating with two artificial breaths, with a speed of 100-120 compressions per minute. The ideal can be considered the speed at which two compressions are performed in one second (i.e. a series of 30 compressions in 15 seconds). Another important nuance in the modern algorithm: it does not matter how many people provide assistance, this does not change the number of compressions and artificial breaths.

As a person who periodically performed the actions described above, I can say that the occupation is extremely tedious, and it makes sense to carry out it often for a long time (until the arrival of an ambulance or the appearance of signs of biological death). Therefore, ideally, to hold such events together or even together, in order to periodically change each other.
Interestingly, most Russian-language videos on YouTube on CPR are made using the old ABC system. The modern CAB algorithm seems to be bypassed, although it has become the norm almost everywhere. One of the best, in my opinion, Russian-language video on resuscitation was made in Kazakhstan:
There are also automatic defibrillators, they can be installed in the subway, at airports and offices. I will not say anything about them, they will tell, they will tell everything themselves.
Airways
After the first series of indirect massage, it is recommended to evaluate the airway patency. Instead of checking, which was in the safar system, in the new algorithm it is recommended to immediately turn the head of the affected person to one side and clean the mouth cavity with something (for example, a handkerchief or a piece of clothing).
After that, it is enough to make one artificial breath (see below) to assess the patency, if there is an excursion of the chest, then the airways are passable. If there is no patency, the air will get into the stomach, it will swell like a ball, causing the epigastrium to increase in volume.
Without intubation or the worst of a laryngeal mask with a combitub it is very difficult to offer something in a similar situation. In order to grab a cubic centimeter of chance, it makes sense to perform Heimlich's technique , to repeat the cleansing of the respiratory tract, thus attempting to restore patency.
Mechanical ventilation - in the mouth, in the nose and in other places.
Mechanical ventilation (ALV) is the most controversial moment in the modern CPR algorithm. I can note that in the first minute after the onset of clinical death, the blood is sufficiently saturated with oxygen to not carry out artificial ventilation at all.
I know from experience that ventilator with oxygen in the first or second minute gives an excellent result, but only in cases when clinical death is caused by respiratory causes, for example, severe poisoning by combustion products. In the case of an electric shock, everything is not so straightforward, since clinical death can occur from both fibrillation and paralysis of the respiratory center.
In this case, chest compressions with indirect massage contribute to passive ventilation. On this basis, some authors do not recommend carrying out mechanical ventilation (at the level of basic activities for people without medical qualifications), but now there is no reliable data that such passive ventilation is sufficient.
So, we will assume that after the airway has been restored, it makes sense to perform artificial ventilation in order to guarantee that the blood is saturated with oxygen. There are 2 classic non-hardware methods of oral ventilation “mouth-to-mouth” and “mouth-to-nose” (the latter is rarely used in cases when there are injuries to the cheeks.
Before carrying out, put a handkerchief on the victim’s mouth, several layers of bandage, etc.). protect yourself from the various nastiness that can be found in his mouth.I suppose few people want to be heroes with tuberculosis or some other miraculous, respiratory transmitted disease.
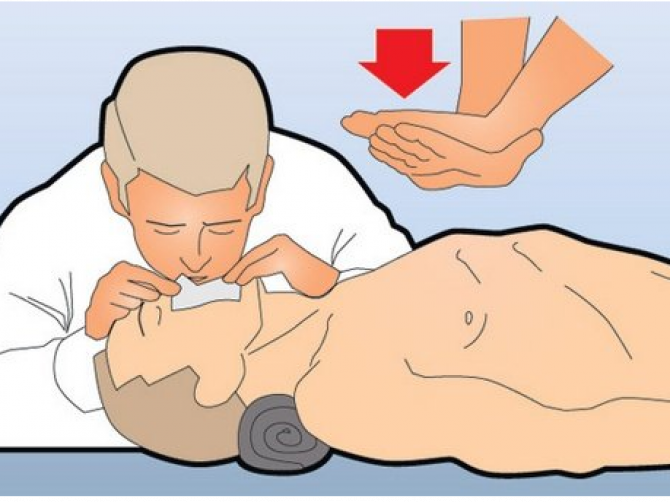
The method of carrying out mechanical ventilation according to the “mouth-to-mouth” method is simple: we take air into the lungs and exhale into the affected person’s mouth, trying to avoid cracks and depressurization. As I have already noted, there should be 30 compressions of indirect massage for two artificial breaths. Ventilation by the “mouth-to-nose” method is carried out similarly, only with the difference that the mouth and the damaged cheeks are sealed (they bury with their hands).
More effective is the use of S-shaped duct, which is not always and not all. It must be entered correctly, as shown in this video:
The most effective method of mechanical ventilation, which can be used by people without medical education, is ventilation with an Ambu bag . The respiratory mask of the bag is pressed against the face of the victim, after which the bag is compressed. But, as a rule, such useful things as the Ambu bag and the S-shaped air duct are not on the scene.
I sincerely hope that the information presented will never be useful to our readers and that they will never fall into a situation in which they will have to apply it in practice. Meanwhile, I am sure that it will not be superfluous - forewarned, it means it is armed. Write about what you think in the comments, maybe I forgot about something, ask questions, try to answer in detail. Photo
content used:
Russian Red Cross
bezperelomov.com
multiurok.ru/files/okazaniie-piervoi-pomoshchi-pri-elieierotravmakh.html
www.passeidireto.com/arquivo/55103532/apostila---o-ambiente-e-as-doencas- do-trabalho / 34
deskgram.net/p/1660912047285500775_6215093419
Advertising load
Let me remind you that we sellelectronics, different, a lot. If you follow the rules of operation, the electronics we sell does not cause an electric shock. Moreover, we do not know of a single case when our customers would receive an electric shock from the goods purchased from us.
At the same time, most people want to clearly understand “how to” and “how effectively”, and not think out and argue about the author of which manual is right and whose teacher. Under the cut, a longrid is waiting for you about first aid for electrical injury with a focus on cardiopulmonary resuscitation (which is most confusing). It will be hard to push everything into one article, so at the moment we will manage first aid for adults, I will dedicate one more material to age features.
For those who are too lazy to read a lot, a section has been created that combines everything written in the most abbreviated form.
First Aid Sequence for Electric Shock
The sequence of actions is the most important thing that you need to know when assisting a person with an electric shock. Electric shock often results in death, and failure to follow the sequence of actions leads to several deaths or serious consequences for several people at once. For example, as happened in Mexico last year in the video below:
The video contains shots that kill people, which may affect the mental state of children and sensitive adults.
The main thing that the described sequence is aimed at is to minimize the probability of hitting the one who is helping. Let's start by the points:
Discharge from the current
Stop the effect of the electric current on the victim by disconnecting the
current source. If it is impossible, remove the conductor from the victim using dry (!) Objects created from dielectrics. It is important to remember that the classic example with a stick or mop, which is in some benefits, is not very good, due to the fact that mops are wet, as well as wood lying on the ground.
Ideally, the use of dielectric gloves, which are considered the ideal way to protect against voltage up to 1 kV, which is consistent with the electrical shock from household appliances and charging gadgets. When talking about a higher voltage, and as a consequence of a more serious current (high-voltage lines, industrial electrical installations, substations), it is necessary to use dielectric bots and a dielectric mat.
In some recommendations it is advised to wear dry wool or household rubber gloves, rubber boots, you can additionally put insulating material (rubber mat, board) under your feet, then remove the conductor from the body with a dry dielectric or clothes
It is also recommended that the victim be struck at least 4-5 meters in case of a household electrical shock (voltage up to 1kV).
If the mains voltage is more than 1 kW (break of a power line wire, for example), if you do not have the appropriate tolerance (and at the same time a set of dielectrics), you should not approach the victim closer than 8 meters. It is necessary to call the Ministry of Emergency Situations and the ambulance, and, if possible, warn others about the danger. On the topic of what is better to remove the conductor from the body of the victim, when there are no special tools, you can write a dissertation. For those who have a great desire to delve into the topic, I recommend first to get acquainted with what electric
Also, in extreme cases, the source can be cut off (for example, wires) with an ax with a dry dielectric handle.
dielectric strength . Understanding the electrical strength of the materials from which the objects around you are made, and knowing the characteristics of the current, you can easily find a suitable object.
It is also important to understand that turning off the source causes the light to go off. This should be taken into account when assistance is provided in the dark or in a room without natural light.
Examination (pulse, respiration, consciousness, bleeding, burns)
After the release of the current, you should call the ambulance and conduct an inspection of the victim. The main thing in this examination is to assess the state of functions, without which the victim can not live - this is blood circulation (pulse first on the carotid, and if available - on the radial artery) and respiration (can be determined by chest excursions, fogging of glasses or mirrors, listening, tactile sensation air movement).
determination of the pulse on the carotid artery
determination of the pulse on the radial artery
Also, during the initial examination, the presence of consciousness is assessed, which is not so important for life, but can provide substantial information about the severity of the victim's condition. You can try to bring the affected to the feelings with the help of ammonia. If, even from a foul-smelling liquid ammoniac, a shock struck did not regain consciousness, then we most likely deal with a severe defeat. In this state, clinical death (cardiac and respiratory arrest) can occur at any time and the victim needs increased attention to his vital functions (pulse, breathing).
Moreover, a number of authors write that after an electric shock there are long-term effects and, against the background of external well-being, cardiac arrest may suddenly develop (which is probably due to the defeat of His bundles). Therefore, it is extremely important to constantly monitor the condition of the affected before the ambulance arrives. Even if he is conscious and looks like a slightly excited "hearty".
If there is no pulse and (or) breathing - talking about clinical death, you must immediately proceed to cardiopulmonary resuscitation (which I will write in detail in the next section). It is important to begin resuscitation in the first minutes after the onset of clinical death (cessation of blood circulation and (or) respiration). After 5 minutes, irreversible changes occur in the cerebral cortex.
Also interesting is the case when the pulse is only on the carotid artery (on the neck), but not palpable on the radial (on the wrist). This is an extremely deceptive state, which indicates decompensated shock and a drop in blood pressure below 60 mm. Hg Art. In such a situation, it is necessary to prepare for cessation of breathing and (or) cardiac activity, after the onset of which it is logical to begin cardiopulmonary resuscitation.
Bleeding
If breathing and pulse is present, it makes sense to pay attention to the presence of bleeding, which sometimes happens with electric shock. Electric shock rarely leads to heavy bleeding, most likely it will be capillary or venous bleeding at the points of entry and exit of the discharge. Venous requires stopping with a pressure bandage. The capillary stop itself, but in order not to infect the wound, you should (if possible) close it with something sterile, for example, a bactericidal adhesive plaster.
Burns
Burns may also be present on the skin. If the burn surface occupies a large area and causes intense pain, it must be cooled with a large amount of water (it is important to do this at a safe distance from the current source). In the future, burns should be possible to close with something sterile, a bandage, for example. It is important not to tear off the pieces of burnt clothing, if any, but to leave them in place by closing the bandage along with the affected tissue.
Fractures and dislocations
As we found out in the previous article, mechanical injuries are quite likely in the event of electric shock, and may appear from both indirect and direct action of the current. That is, if the affected person did not fall from a height and did not beat all parts of the body against the floor, this does not mean that he cannot have a fracture or dislocation.
On examination of a fracture, there may be evidence of tissue swelling, limb deformity, a hematoma at the fracture site, and pain itself. About sprains usually says pain, pathological (not normal) mobility in the joint, deformity in the joint area. Fractures and dislocations must be immobilized - that is, immobilize, most likely an ambulance will do this. If you intend to encounter a mechanical injury if an electric shock occurs outside the exit area of an ambulance brigade, read more about transport immobilization.
General events
Also, the affected person must be drunk hot (not to be confused with feverish), give a blanket (avoid heat loss as in a state of shock), and offer validol as a placebo. It is also important to provide psychological rest, if the injured core with arrhythmia and complains of an attack, you should help him find antiarrhythmic, prescribed by a doctor, which may be with him or nearby.
CPR
Flour choice. And which algorithm is correct?
With this theme, too, things are not as simple as they seem. Perhaps everyone has seen how the films perform indirect heart massage, while the passionate rescuers of Malibu conduct intensive and seductive artificial ventilation of the lungs by mouth-to-nose method (cross out) in the mouth. Some, probably, also managed to notice that in all films this is done differently and in most cases wrong.
All drivers were taught in driving schools the skills of elementary resuscitation, as a rule, according to the method of Peter Safar (Peter Safar), better known as ABCD. At the same time, the overwhelming majority of drivers managed to forget about what the letter combination means. Other people have been trained in different places and at different times and may know other techniques. For example, doctors who studied in the harsh 90s recall the Russian “UNIVERSAL” algorithm, someone remembers unnamed Soviet norms based on the same Safara, etc. However, when it comes to business, there is a stupor and a misunderstanding of how best to do it.
In 2010, when CPR by Safar turned 50 years old and in the same year, it was finally recognized as ineffective by modern standards, replacing it with a more advanced algorithm. In this regard, I strongly recommend that you forget everything that you remembered before and pay attention to what is accepted today by WHO and AKA (American Heart Association). In this article we will look at the CAB algorithm. I will write below about the features of the latest version of this algorithm (in a form adapted for people without special medical knowledge).
Who has a great desire to learn about the evolution of ideas about CPR, can read this article.
CAB is our all
Order of letters in the abbreviation CAB indicates the sequence in which resuscitation actions are performed:
- C - circulation (circulation) - indirect heart massage (in some recommendations - precordial stroke);
- A - airways (airways) - restoration of airway patency (if there are problems with it);
- B - breathing (breathing) - artificial ventilation of the lungs.
The preparatory stage
Affected (which is already removed at a sufficient distance from the current source) should be laid on a hard, flat, dry surface. It makes sense to put something under his legs, to free him from clothes that prevent assistance. It is allowed to take off / unfasten / tear / cut clothes that make it difficult to access the chest. In this case, history knows cases when even paramedics presented financial claims for expensive linen. In this regard, some authors clarify that if you can quickly unbutton it is better to unbutton it and not cut it. After the preparatory phase, you can begin resuscitation.
Precordial punch: optional, dangerous, optional
Such a blow is the only method of mechanical defibrillation and can be effective due to the genesis of clinical death (which is often caused by fibrillation in electric shock). The automatic defibrillator is much more efficient, but, unfortunately, is not available everywhere.
Due to the trauma and high risk, the precordial blow is not used by the volunteers of the National Red Cross societies , and it was also removed from international recommendations and benefits.
At the same time, the method proved its effectiveness in the first seconds during fibrillation. To be objective, I will describe the method of application, with the proviso - the technique is really traumatic, is not included in modern algorithms for CPR, and it is the person who provides assistance for the consequences of its application.
The blow should be applied in case of a 100% certainty that there is no blood circulation, no pulse, and cardiac arrest occurred before your eyes. If you are not sure of the correctness of the strike - do not apply it and proceed to an indirect heart massage. The blow is applied with the edge of the palm clenched in the fist across the sternum, the blow must fall into place 2 centimeters above the xiphoid process of the sternum (that is, where shown in the figure). The xiphoid process itself must be palpated (grope) and be sure to close with your fingers. Only then can one strike (!) A sharp blow above the fingers (covering the process) from a distance of no more than 20 cm.
No need to bash on the sternum with all the dope in a fit of insane heroism. You can not beat from the shoulder , the main thing is not strength, but how sharply the blow is dealt. It is important to understand that during the resuscitation, the carer has a lot of adrenaline and remarkable strength appears even in fragile-looking girls.
Indirect massage - correctly 30, not 10-15
Indirect massage is the most statistically effective method of elementary cardiopulmonary resuscitation and is a compression in the same place in which the precardiac stroke was performed - strictly in the middle of the chest, 2-3 centimeters above the xiphoid process . It is important not to move your hands to the right or left, in such cases it is easy to damage the ribs, and the rib cage fragments of the ribs are easily damaged.
Location of an indirect massage
Compression when performing an indirect massage is performed with the base of the palm of one hand, the other presses from above, the fingers are raised to eliminate pressure on the ribs. The important point is that the arms should be straightened, flexion in the elbows is not allowed. The depth of the compression movements should be 5 cm. At this depth, it is possible to squeeze the heart to provide sufficient blood pressure to supply blood to the brain.
There is a lot of discussion about the frequency with which compression should be performed. Modern algorithms assume a series of 30 compressions alternating with two artificial breaths, with a speed of 100-120 compressions per minute. The ideal can be considered the speed at which two compressions are performed in one second (i.e. a series of 30 compressions in 15 seconds). Another important nuance in the modern algorithm: it does not matter how many people provide assistance, this does not change the number of compressions and artificial breaths.
As a person who periodically performed the actions described above, I can say that the occupation is extremely tedious, and it makes sense to carry out it often for a long time (until the arrival of an ambulance or the appearance of signs of biological death). Therefore, ideally, to hold such events together or even together, in order to periodically change each other.
Interestingly, most Russian-language videos on YouTube on CPR are made using the old ABC system. The modern CAB algorithm seems to be bypassed, although it has become the norm almost everywhere. One of the best, in my opinion, Russian-language video on resuscitation was made in Kazakhstan:
There are also automatic defibrillators, they can be installed in the subway, at airports and offices. I will not say anything about them, they will tell, they will tell everything themselves.
Airways
After the first series of indirect massage, it is recommended to evaluate the airway patency. Instead of checking, which was in the safar system, in the new algorithm it is recommended to immediately turn the head of the affected person to one side and clean the mouth cavity with something (for example, a handkerchief or a piece of clothing).
After that, it is enough to make one artificial breath (see below) to assess the patency, if there is an excursion of the chest, then the airways are passable. If there is no patency, the air will get into the stomach, it will swell like a ball, causing the epigastrium to increase in volume.
Without intubation or the worst of a laryngeal mask with a combitub it is very difficult to offer something in a similar situation. In order to grab a cubic centimeter of chance, it makes sense to perform Heimlich's technique , to repeat the cleansing of the respiratory tract, thus attempting to restore patency.
Mechanical ventilation - in the mouth, in the nose and in other places.
Mechanical ventilation (ALV) is the most controversial moment in the modern CPR algorithm. I can note that in the first minute after the onset of clinical death, the blood is sufficiently saturated with oxygen to not carry out artificial ventilation at all.
I know from experience that ventilator with oxygen in the first or second minute gives an excellent result, but only in cases when clinical death is caused by respiratory causes, for example, severe poisoning by combustion products. In the case of an electric shock, everything is not so straightforward, since clinical death can occur from both fibrillation and paralysis of the respiratory center.
In this case, chest compressions with indirect massage contribute to passive ventilation. On this basis, some authors do not recommend carrying out mechanical ventilation (at the level of basic activities for people without medical qualifications), but now there is no reliable data that such passive ventilation is sufficient.
So, we will assume that after the airway has been restored, it makes sense to perform artificial ventilation in order to guarantee that the blood is saturated with oxygen. There are 2 classic non-hardware methods of oral ventilation “mouth-to-mouth” and “mouth-to-nose” (the latter is rarely used in cases when there are injuries to the cheeks.
Before carrying out, put a handkerchief on the victim’s mouth, several layers of bandage, etc.). protect yourself from the various nastiness that can be found in his mouth.I suppose few people want to be heroes with tuberculosis or some other miraculous, respiratory transmitted disease.
The method of carrying out mechanical ventilation according to the “mouth-to-mouth” method is simple: we take air into the lungs and exhale into the affected person’s mouth, trying to avoid cracks and depressurization. As I have already noted, there should be 30 compressions of indirect massage for two artificial breaths. Ventilation by the “mouth-to-nose” method is carried out similarly, only with the difference that the mouth and the damaged cheeks are sealed (they bury with their hands).
More effective is the use of S-shaped duct, which is not always and not all. It must be entered correctly, as shown in this video:
The most effective method of mechanical ventilation, which can be used by people without medical education, is ventilation with an Ambu bag . The respiratory mask of the bag is pressed against the face of the victim, after which the bag is compressed. But, as a rule, such useful things as the Ambu bag and the S-shaped air duct are not on the scene.
Briefly about the most important for those who are lazy to read
- Turn off the current before assisting. If you can not turn off, remove the current source from the victim, using dry dielectric objects, rubber as possible, ideally, special dielectric gloves, carry the victim away (5 m - household network, 10 m - industrial or power lines).
- Call an ambulance. We evaluate the pulse, breathing and consciousness at the same time. If there is no pulse and breathing, we begin reanimation. If there is - determine the presence of mechanical injuries and wounds.
- Resuscitation is performed using the CAB algorithm. If you are not sure that you can deliver a precordial blow correctly - we don’t use it (if you are a Red Cross volunteer - we don’t use it anyway). We combine 30 chest compressions with two artificial breaths.
- Burns are closed with a sterile dressing, after cooling the burn surface with water.
- Venous bleeding is stopped by a pressure bandage, capillary - we close the aseptic.
- Mechanical injuries immobilized, better tires.
- Provide the victim with rest, give a blanket, give a drink of hot and watch for his condition.
Total
I sincerely hope that the information presented will never be useful to our readers and that they will never fall into a situation in which they will have to apply it in practice. Meanwhile, I am sure that it will not be superfluous - forewarned, it means it is armed. Write about what you think in the comments, maybe I forgot about something, ask questions, try to answer in detail. Photo
content used:
Russian Red Cross
bezperelomov.com
multiurok.ru/files/okazaniie-piervoi-pomoshchi-pri-elieierotravmakh.html
www.passeidireto.com/arquivo/55103532/apostila---o-ambiente-e-as-doencas- do-trabalho / 34
deskgram.net/p/1660912047285500775_6215093419
Advertising load
Let me remind you that we sellelectronics, different, a lot. If you follow the rules of operation, the electronics we sell does not cause an electric shock. Moreover, we do not know of a single case when our customers would receive an electric shock from the goods purchased from us.