CBT: psychotherapy for geeks
When it comes to psychotherapy, many imagine the legendary couch, the twilight of a cozy office, the wise elderly therapist with a cigar and endless associations: “ you know, yesterday I saw a man with an umbrella on the street, he walked so fast that his umbrella swayed evenly and this caused I have some vague, vague feelings in me, he reminded me of my older brother Ivan, with whom we played doctor as a child, he, by the way, has now become so much like his father! "
Others immediately begin to recall non-falsifiability (Popper unscientific), the absence of a sound evidence base regarding the clinical effectiveness of such conversations, cases of many years of analysis (and psychoanalytic literature describes the experience of interaction between a client and an analyst that consists of dozens of years of regular paid meetings), reluctance to use Occam's razor and other unpleasant things.
Today I want to talk with you about CBT and show that psychotherapy may well be different.
Tl; dr: The article describes the basics of CBT. If you have psychological problems, but you do not believe that they can be solved by talking about how your mother did not like you in childhood, you may like this area of psychotherapy. It is logical, rational and almost without unnecessary entities. And most importantly - focuses on thoughts, not feelings.
Comparison with Psychoanalysis
It so happened that so far among non-specialists, psychotherapy as such is often associated with one particular direction of it - psychoanalysis (in the West, by the way, on the contrary, psychotherapy by default is CBT). And all the stereotypes mentioned above are either generated by him or relate, for the most part, to him (and to some derivative psychodynamic directions).
So, the first difference between CBT and psychoanalysis is, paradoxically, the name. The first is cognitive-behavioral therapy , i.e. therapy aimed at changing how a person thinks (his thoughts), and how he behaves. The second, as the name implies, claims to work with the psyche in all its complexity and diversity.
The second difference is that a lot of things are postulated in psychoanalysis: dividing the psyche into Eid (“a place where instincts, animal desires and impulses seethe”), Super-Ego (according to the ideas of psychoanalysts, moral attitudes of a person are stored and act) and the Ego (a structure that ensures that the interests of the Eid are respected while observing the prohibitions of the Super Ego).
CBT does not tell us anything about how the psyche “really” works, it simply works with its observable (externally or by introspection) phenomena.
Psychoanalysis tells us about libido - a kind of motive energy of the psyche (which no one has ever seen), to which, allegedly, one can reduce all the motives of human aspirations and actions. CBT is looking for specific reasons for each particular case, not trying to find the ultimate basis.
In psychoanalysis, the main emphasis is on the work of the so-called "Unconscious", all the causes of neurosis and ways to solve them, from his point of view, are there: you need to get the client into the unconscious part of the psyche in a roundabout way, release the repressed needs and everything will be OK. What the client thinks is interesting for the psychoanalyst only insofar as these thoughts can lead him to ideas about what is happening in the unconscious.
In CBT, the therapist is directly interested in the client’s thoughts and believes that it is thoughts and behavior, and not semi-mythical unconscious entities, determine the well-being and degree of adaptation of the client to the environment.
Psychoanalysis is a fundamentally long-term method of work. First you need a long period of establishing rapport, then a transfer should develop to the analyst (a state in which, supposedly, the client transfers his relations from early childhood (not always, but most often) to the analyst, for example, trying to get his love, as he did with Mother).
In CBT, there are simple and understandable learning relationships: the therapist teaches the client to think and act in a more healthy and adaptive way. And the duration of therapeutic contact is recommended to be limited, for example, to thirty sessions (this is a lot, but much less than with psychoanalysis).
Finally, ideologically, psychoanalysis focuses on what happens in the hypothetical internal structures of the client’s psyche, and CBT on how the client manifests himself in the world.
Efficiency and scope of CBT
Traditional CBT has limitations on its use - it gives the best effect for anxiety disorders and depressions of a neurotic level (the term, by the way, is from psychoanalysis), i.e. with relatively mild cases of disturbance. Although, for example, severe psychotic depressions, anxiety disorders, eating disorders and even obsessive-compulsive disorders are quite amenable to correction with its help.
To work with patients with a large degree of disturbance, special types of therapy have been developed, which, however, are close to CBT ideologically and, in many ways, are based on it:
1. Young chemotherapy - added features from other areas of psychotherapy, in particular, transactional analysis and gestalt;
2. Dialectical behavioral therapy Linehan - expanding CBT to work with borderline personality disorder, added anger management and a bunch of other interesting things;
3. Functional and analytical therapy of Cochlenberg and Tsai - focus shifting from the cognitive to the behavioral;
4. And even mind-based cognitive therapy of Segal and Williams is an infernal mixture of Buddhist practices and CBT;
But we will not consider them in detail in the framework of this article, but rather talk about what data we have regarding the effectiveness of classical CBT.
Beck's first classic article [1] came to mind, which showed greater efficacy of CBT compared with pharmacotherapy (the classic tricyclic imipramine, an analogue of the well-known amitriptyline to the general public, was used).
By the way, a more modern meta-study shows that CBT can be more effective than drug treatment when working with children and adolescents suffering from obsessive-compulsive disorder [5].
Further, one can recall a rather large review from 2010 [2], which showed a higher (compared with other types of psychotherapy) effectiveness of CBT in anxiety and depressive disorders.
The experts of the French National Institute for Health and Medical Research (INSERM) in their meta-analysis recognized the effectiveness of CBT in the following types of disorders [3]: agoraphobia, panic disorders, generalized anxiety disorder, sociophobia, post-traumatic syndrome, obsessive-compulsive disorder, depression (mild forms and depression moderate severity), bipolar affective disorder, schizophrenia (a chronic form in combination with antipsychotics), borderline personality disorder, avoiding disorders in person, etc.
It is important to note that CBT is an effective way to combat anxiety not only in adults, but also in children and adolescents [4].
Another feature of CBT is that it is effective not only in the format of the classic face-to-face work with a psychotherapist, but also with the provision of therapeutic care remotely (ie via the Internet) [6,7].
And the most interesting thing for us: there is evidence [8] that, at least in some cases and situations, CBT can be applied to oneself, without the participation of a therapist. It should be noted here that, unlike classical psychoanalysis (I know that in some psychodynamic schools this is also allowed, but this is not about them), a rather significant (if not to say, large) part of the work is carried out by the client independently, even if he works with the therapist. CBT is not the case when the therapeutic process occurs one hour once a week, the client has to work very intensively on himself between sessions.
CBT Basics
As its name implies, cognitive-behavioral therapy is built around two things: how the client thinks, and how he behaves.
CBT is based on the assumption that what happens to a person depends to a large extent on how he structures the world. And this is determined by the way he thinks. In CBT, unlike many other psychotherapeutic approaches, it is postulated that human thoughts evoke emotions , and not vice versa.
The so-called. automatic thoughts- this is, oddly enough, thoughts that appear automatically. Let us explain an example: during the writing of this article, the author had to distract for several days to solve some domestic problems. When he found out about this, a whole series of involuntary and, as further analysis showed, destructive thoughts such as “ I am a loser ”, “ I won’t succeed ”, “ I am thrown out of GeekTimes ” and the like, arose in his brain .
Automatic thoughts are not always destructive; moreover, they are not always incorrect. But one should treat them with suspicion - as a rule, they are the offspring of the principle of saving resources: the brain is “lazy" to calculate the situation completely and issues the first decision / judgment. And it often happens that the same brain, if you make it think carefully, will give a completely different assessment or make a completely different decision.
For example, a person who grabs minuses into karma may automatically consider himself flawed, but if he thinks well, he will understand that he simply made too harsh and erroneous statements (a single mistake does not prove the flaw of the person who committed it).
A synonym for the term “automatic thought” is the word “ cognition ”.”, Which Beck defined as follows:“ Cognition is a thought or figurative representation that may go unnoticed by you if you do not concentrate on them ”[9].
Actually, that part of the CBT that is cognitive is about teaching the client to catch his cognitions, be aware of them, check for adequacy and (if necessary) replace them with more adequate thoughts. Those. argue with yourself. And no, this is by no means schizophrenia, it is part of the therapeutic process in CBT, called dispute.
Part cognitions contested therapist, part (it must be said - used on most of the) client.
But in CBT there is also a second part - behavioral. A directive approach works here, when the therapist forces the client to behave in a healthy way, for example, a depressed client who lies in bed most of the day will receive a task to draw up (and then to execute) a certain daily routine, including a certain level of activity, and the client with agoraphobia (after appropriate preparation, of course) will be forced to visit crowded places.
Speaking of “appropriate training.” Within the framework of behaviorism (on which the behavioral part of CBT is built) various techniques are possible, but two of them deserve special attention and inclusion in this article.
The first one is with hematological desensitization. Especially good for all kinds of phobias. At the first stage, the client is taught some relaxation technique (muscle relaxation, breathing exercises, etc.), after which they are presented with a stimulus that causes fear.
If we imagine that our hypothetical client is afraid of spiders, then they will show him a photograph of the spider and ask them to use the previously learned technique to relax. When the photo ceases to impress, he will be presented with a spider in the bank at a considerable distance and asked to relax. As you advance in therapy, the incentive will increase until the client loses sensitivity to it.
The second technique is the so-called flood technique. It is inherently the opposite of the first: a person is immediately presented with a stimulus of very high strength and they wait until he gets so fucked up so that he "gets tired of fear."
That, in fact, is the whole point of CBT. Of course, there are many interesting technical aspects, but their consideration is clearly beyond the scope of our review article, and instead of going into these jungles that are understandable only to professionals, we will talk a little more about cognitions, and then consider an example of working with them.
Cognitive errors
Cognitive mistakes are what make our cognitions wrong. Again, not every cognition is erroneous, but those that are not erroneous do not interest us and, accordingly, will not be considered.
Here are some common cognitive errors. Firstly, it is, of course, catastrophic , which consists in the fact that the subject, on the basis of one unsuccessful experience, concludes that " everything is bad and we will all die ." For example, a student who does not pass one exam at a session may not think about how to get a retake, but imagine a terrible future, where he will be taken into the army, he will go to war, he will be taken prisoner, etc. Such thoughts will be absolutely disorganizing and obviously will not help to get out of the situation.
The second interesting and common mistake is over-generalization ( over-generalization ). In this case, a person, ignoring the knowledge gained at the Terver and Matstat courses, makes assumptions about the general population from one fact. And this combination often turns out (in his head, of course) to be hostile, unpleasant and in every possible way threatening the subject. At the programmer, the testers found one non-critical bug, and he is already thinking about leaving the profession, since he was a quick-coder and a bag-maker - this is it.
One of my favorite cognitive mistakes is the so-called. “ Tyranny of longevity ”, which is based on three pillars: “ I owe ”, “ they owe me ”, “the whole world owes me". Let's look at some examples to make it clearer.
The enikeyschik in the company regularly participates in the inventory of goods, even when there is no direct order from the director, but only the insistent demand of the head of the logistics department. Why? Because he feels that he should do it, although in reality there is no obligation relationship: it is not spelled out in the contract, there is no order of the head, there is only a cognitive distortion: " I have to, otherwise they will fire me ."
Another example: the subject requires something that was not agreed upon. A mother requires her son to enter the chosen specialty (“ you must become a doctor»), The boss demands that the subordinate clean the office premises, very surprised and indignant that the latter himself had not thought of this. “But this is elementary, he should have guessed!”
An example of the third type of longevity: a girl experiences great distress from the fact that the bus did not arrive on the route that she needed (" How so, everything should be in my opinion! ").
The examples may seem exaggerated, but they are all taken from real life, and not one of them is invented. By the way, if you have not read the Wikipedia article on cognitive bias , I recommend it.
How does work with a therapist work?
Imagine that you wanted to try CBT on yourself. How will it look like? First you will look for and select a therapist (a separate and rather voluminous topic), then conclude a therapeutic contract with him and, possibly, a contract for changes, after which, in fact, the main work will begin.
Beck himself wrote that the therapist must teach the client how to solve the following problems [9]:
1) track your negative automatic thoughts (perceptions); 2) recognize the relationship between their own thoughts, emotions and behavior; 3) to analyze the facts confirming or refuting his views; 4) to develop more realistic assessments and perceptions; 5) identify and modify dysfunctional beliefs predisposing him to distort experience.
First, the client will be told about cognition, after which a certain amount of time will be spent on the practice of tracking them and determining their effect on the emotional background and behavior.
Then the fun part begins - an assessment of the adequacy of cognition and what is called a "dispute" in the CBT - challenging inadequate and destructive automatic thoughts.
This can be done in different ways: bring proof to scientific research, find logical contradictions in client's conclusions, conduct an experiment. The experiment , in the opinion of the author, is the most powerful technique. So, for example, if a person is afraid to assert his rights and even simply express his opinion in a team, believing that everyone will immediately turn away from him, then the opposite behavior can be suggested as an experiment.
Often, the results of an experiment differ so much for the better from the client’s expectations that the latter takes the experimental model of behavior as the main one. So, for example, one girl who was afraid to defend her opinion, not only did not lose her position in the team, but was also able to gain a higher position in the informal hierarchy, significantly reducing the background level of frustration.
What does a dispute look like without experiment? I will give an example from my own therapy:

Here I could not cope without pharmacotherapy, but still it was an important step towards recovery.
The second situation, not complicated by pharmacology, is for analysis:
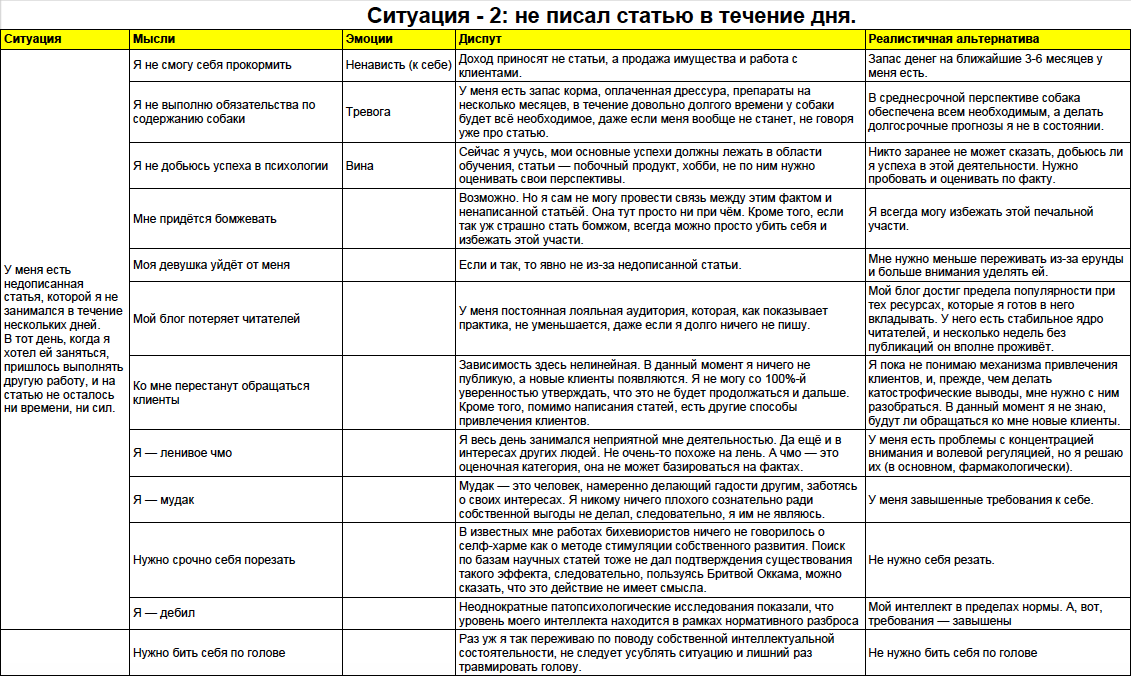
Actually, the reader will have to deal with compiling such (or similar) tablets if he decides to work on the CBT basis.
It is believed [9] that in the process the brain trains, as it were, and over time, inadequate and destructive automatic thoughts will be replaced by more adequate and constructive ones. Clinical proofs of the effectiveness of this technique are given above.
Of course, the CBT is not limited to the elementary techniques presented here - there is identification and development of deep destructive installations, work with the management of aggression, and much more, but we will consider all this in the following articles if the topic itself turns out to be interesting to the community.
Literature
1. Augustus J. Rush, Aaron T. Beck, Maria Kovacs, Steven Hollon. Comparative efficacy of cognitive therapy and pharmacotherapy in the treatment of depressed outpatients. Cognitive Therapy and Research. March 1977, Volume 1, Issue 1, pp 17–37
2. David F. Tolin. s cognitive – behavioral therapy more effective than other therapies ?: A meta-analytic review. Clinical Psychology Review. Volume 30, Issue 6, August 2010, Pages 710–720
3. INSERM Collective Expertise Center. INSERM Collective Expert Reports [Internet]. Paris: Institut national de la santé et de la recherche médicale; 2000-. Psychotherapy: Three approaches evaluated. 2004. Available from: www.ncbi.nlm.nih.gov/books/NBK7123
4. Cochrane evidence. Cognitive behavioural therapy for anxiety in children and young people.
www.cochrane.org/CD004690/DEPRESSN_cognitive-behavioural-therapy-for-anxiety-in-children-and-young-people
5. Cochrane evidence. Behavioural and cognitive-behavioural therapy for obsessive-compulsive disorder (OCD) in children and adolescents.
www.cochrane.org/CD004856/DEPRESSN_behavioural-and-cognitive-behavioural-therapy-for-obsessive-compulsive-disorder-ocd-in-children-and-adolescents
6. Cochrane evidence. Internet-based cognitive behavioral therapy with therapist support for anxiety in adults: a review of the evidence.
www.cochrane.org/CD011565/DEPRESSN_internet-based-cognitive-behavioural-therapy-therapist-support-anxiety-adults-review-evidence
7. Cuijpers, P., van Straten, A. & Andersson, G. J Behav Med ( 2008) 31: 169. doi: 10.1007 / s10865-007-9144-1
8. A Randomized Controlled Trial of Self-Directed Versus Therapist-Directed Cognitive-Behavioral Therapy for Obsessive-Compulsive Disorder Patients With Prior Medication Trials. Behavior Therapy, Volume 38, Issue 2, Pages 179-191
David F. Tolin, Scott Hannan, Nicholas Maltby, Gretchen J. Diefenbach, Patrick Worhunsky, Robert E. Brady
9. A. Beck, A. Freeman. Cognitive therapy for depression.